Lumbar fusion surgery involves various methods of “fusing” one spinal vertebra to another. The two bones grow together, or “fuse” together. This process often takes 6- 12 months, which is why I routinely explain to my patients that a fusion surgery is really two parts: The first is what we do in the operating room, decompressing the nerves and placing the instrumentation. The second is what the patient’s body does over the following months, where the tissues and bones heal… or don’t heal.
When the bones do not fuse, this is typically called “non-union” or pseudoarthrosis. Rates of lumbar pseudoarthrosis range anywhere from 5% to 35%, with a higher incidence when more levels are involved, and a significantly higher incidence with 3 or more levels.
Pseudoarthrosis can be asymptomatic. Not all patients who do not fuse develop symptoms, and therefore sometimes “non-union” can be observed. Furthermore, pain and symptoms following a fusion surgery do not always mean a pseudoarthrosis has occurred. Lastly, pain or other symptoms in the presence of a pseudoarthrosis, may be related to the pseudoarthrosis or something else.
If surgery is required to treat a pseudoarthrosis, the question becomes where to go. Should the patient return to their original surgeon or seek another opinion?
A recent paper was published in Neurosurgery, addressed this question by looking at lumbar fusions revised by the same or different surgeon. Although not exactly clear why, there was a trend for a better outcome when revision surgery was performed by a different surgeon.
Likely, part of the explanation lies is in “how” a revision surgery is performed. If a revision is performed simply by repeating the same surgery again, the result may not change (this is not uniformly true). However if the revision surgery takes a different perspective, then maybe there’s a better outcome of fusion (this is not uniformly true).
Take these two case examples:
 Case 1
Case 1
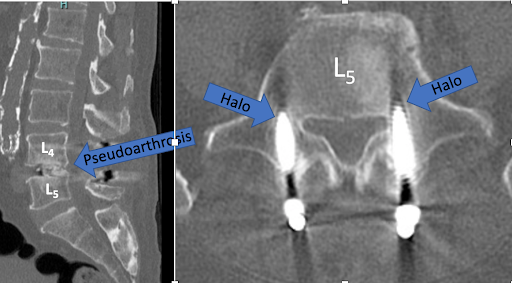
One surgeon performs a standard posterior interbody fusion at L4-5. Over time, symptoms return and a CT scan shows a pseudoarthrosis. The patient went to their original surgeon, who recommended just placing larger screws in the back. Then the patient went to a different surgeon, who recommended a new perspective.
 This surgeon offered a cage/ plate in the front, and then larger screws in the back with more bone added posterolaterally. Even on the intraoperative x-ray from the revision surgery (far right two pictures), more bone can be seen. Time will tell if fusion occurs from a different surgeon’s revision, but it seems like another perspective may offer a good chance.
This surgeon offered a cage/ plate in the front, and then larger screws in the back with more bone added posterolaterally. Even on the intraoperative x-ray from the revision surgery (far right two pictures), more bone can be seen. Time will tell if fusion occurs from a different surgeon’s revision, but it seems like another perspective may offer a good chance.
Case 2
 One surgeon performs a standard posterior interbody fusion at L4-5. Over time, symptoms return and a CT scan shows a pseudoarthrosis.
One surgeon performs a standard posterior interbody fusion at L4-5. Over time, symptoms return and a CT scan shows a pseudoarthrosis.
However, this patient went back to the original surgeon, who simply added larger screws from the back and extended the fusion up and down a level. Minimal bone was placed. This was essentially repeating the same perspective of the initial procedure.
This unfortunately led to the same outcome… pseudoarthrosis.
 Conclusion
Conclusion
Let’s be clear, pseudoarthrosis can occur for a variety of reasons, and is not necessarily related to a patient or their surgeon. Sometimes even in the best of scenarios, pseudoarthrosis occurs and revision surgery is needed.
And that revision surgery does not mean anterior/ posterior revision is indicated or necessary. However, if an initial surgery fails, it may be wise to at least consider another surgeon’s perspective.





