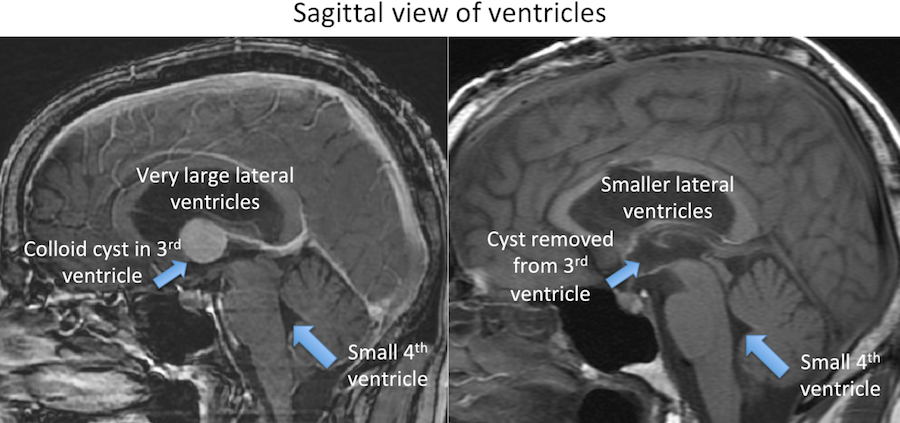
Hydrocephalus results when this fluid cannot normally circulate (becomes blocked) in the brain or when this fluid is not absorbed correctly. The build up of CSF increases the pressure in the brain and can cause symptoms. This usually manifests with the ventricle(s) enlarging. Hydrocephalus can occur at any age.
When something blocks the flow of CSF, we commonly call this “obstructive hydrocephalus”. A cyst or tumor in the ventricles can block the CSF flow. Another common blockage site is the cerebral aqueduct, which sometimes is abnormally small since birth.
When the CSF is not adequately absorbed, we commonly call this “communicating hydrocephalus”. Infection, a brain bleed, or other conditions can lead to “communicating hydrocephalus”.
It is important to understand that an enlarged ventricle size does not always mean hydrocephalus is present. As we age, our ventricles can become enlarged without elevated CSF pressure. This does not always need treatment.
Additionally, pressure can build in our brains without enlarged ventricle size. A condition called, “pseudotumor cerebri” occurs when increased pressure is present with normal or even small ventricles.