Lumbar decompression is one of the most common procedures performed in the lumbar spine.
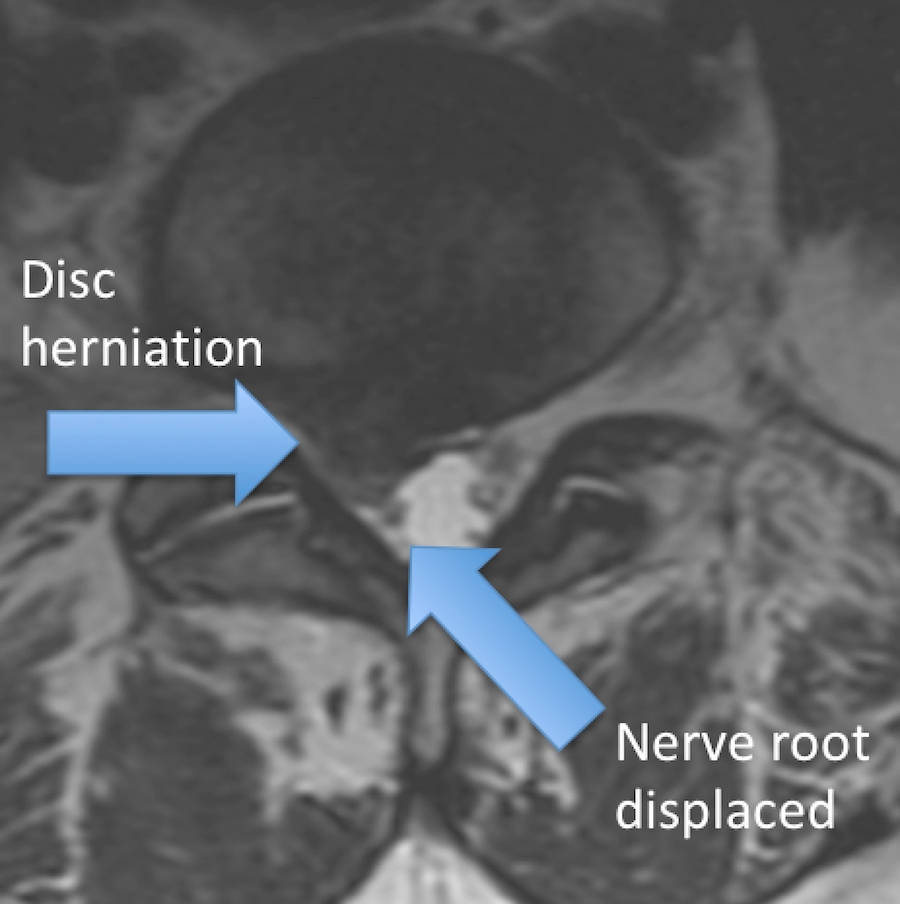
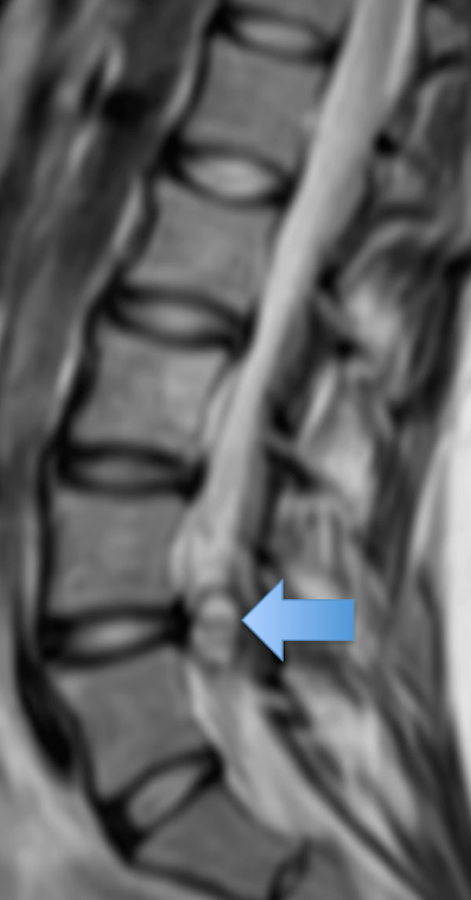
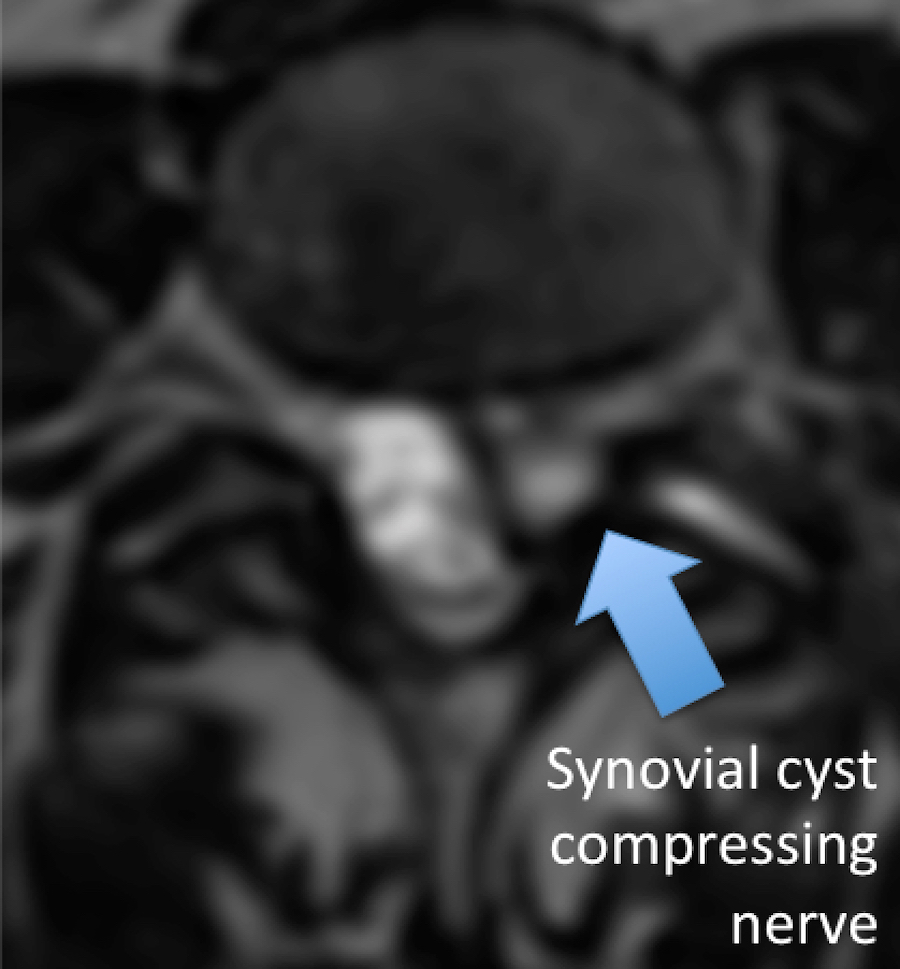
Pressure on the nerves in the low back can occur from multiple factors. The adjoining pictures display the following:
Lumbar decompression is one of the most common procedures performed in the lumbar spine.
Pressure on the nerves in the low back can occur from multiple factors. The adjoining pictures display the following:
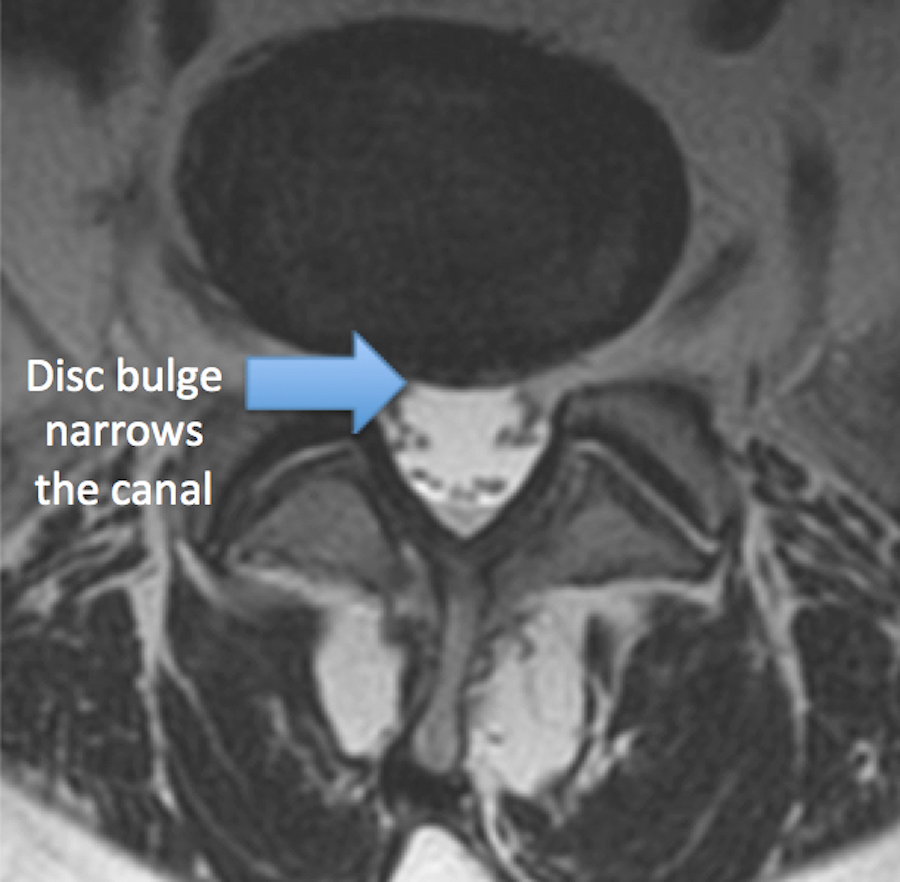

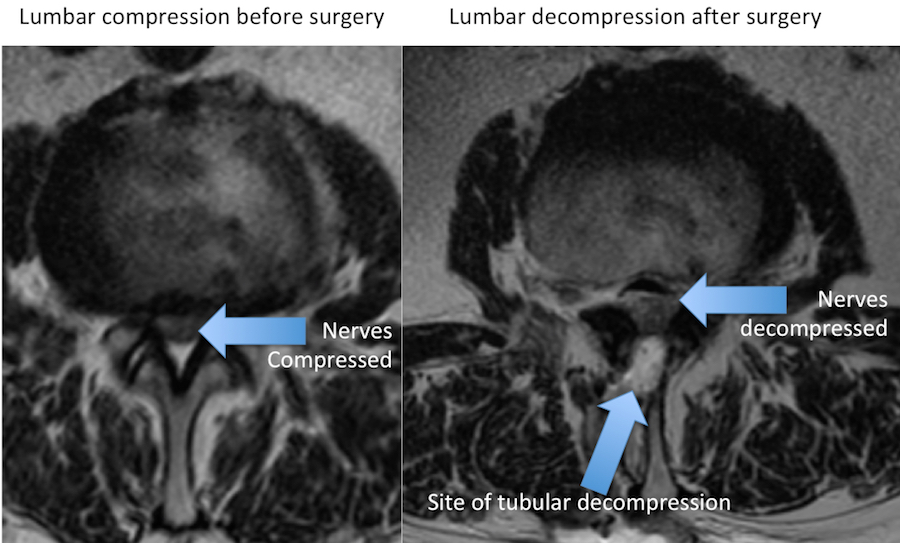
Narrowing of the lumbar spine canal and pressure on the nerves most commonly causes leg symptoms, including pain down the leg (radiculopathy or “sciatica”), leg/foot weakness, or leg/ foot numbness and tingling. Sometimes back pain can also occur.
The initial treatment of back or leg symptoms is often conservative. Observation with or without over-the-counter anti-inflammatories or tylenol may be tried. Sometimes patients try chiropractors or acupuncture. With persistent symptoms, therapy may be the next option. If after a few weeks symptoms are still intractable, then advanced imaging like a spine x-ray or spine MRI may be pursued. If the MRI shows nerve compression, an injection may be tried.
Usually conservative options are tried before considering surgery. In certain circumstances, imaging and surgery are sought sooner. Lumbar decompression may be a good option when the nerves are being compressed and no spinal instability is seen. Lumbar decompression may be performed as an open procedure, but often minimally invasive tubular lumbar decompression can be a better option.
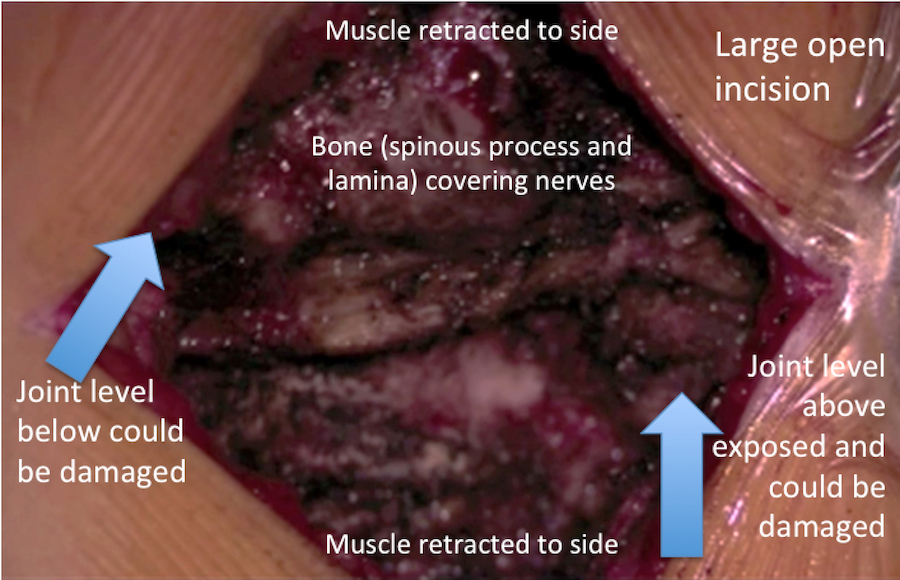
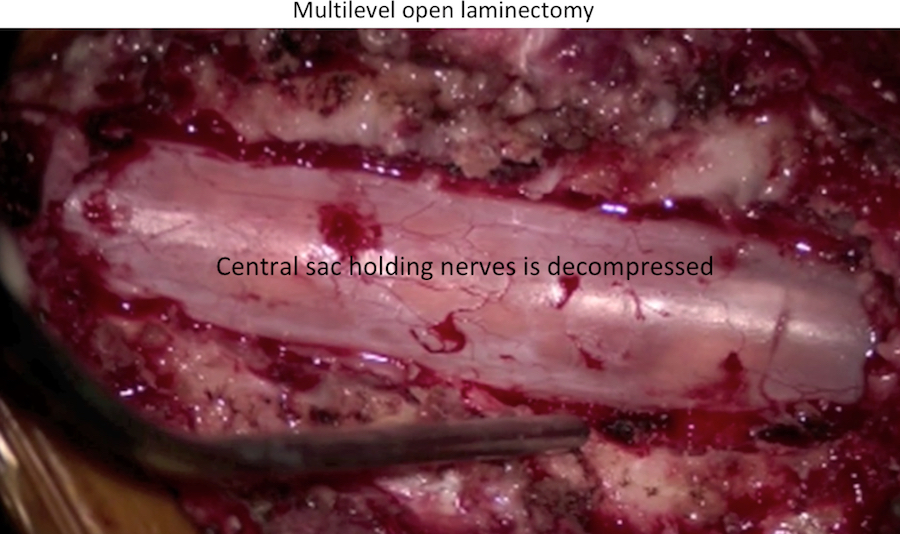
In an open lumbar decompression, the muscles are ripped off the lumbar bones and held open with retractors. This may lead to more muscle damage, as well as damage to the joints above and below the level of surgery.



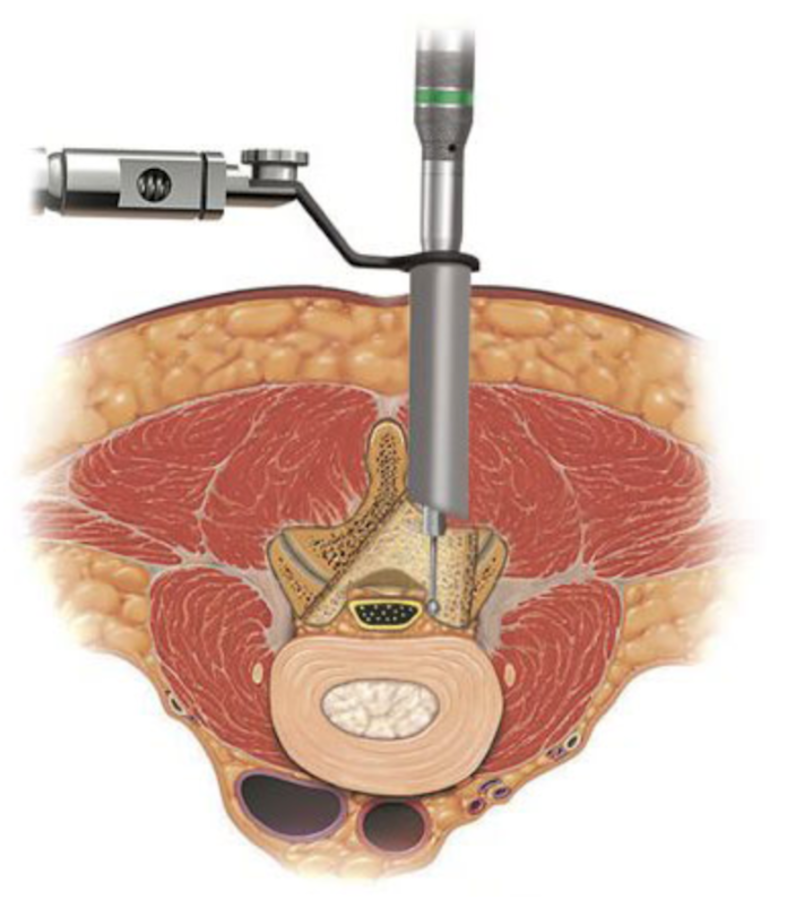
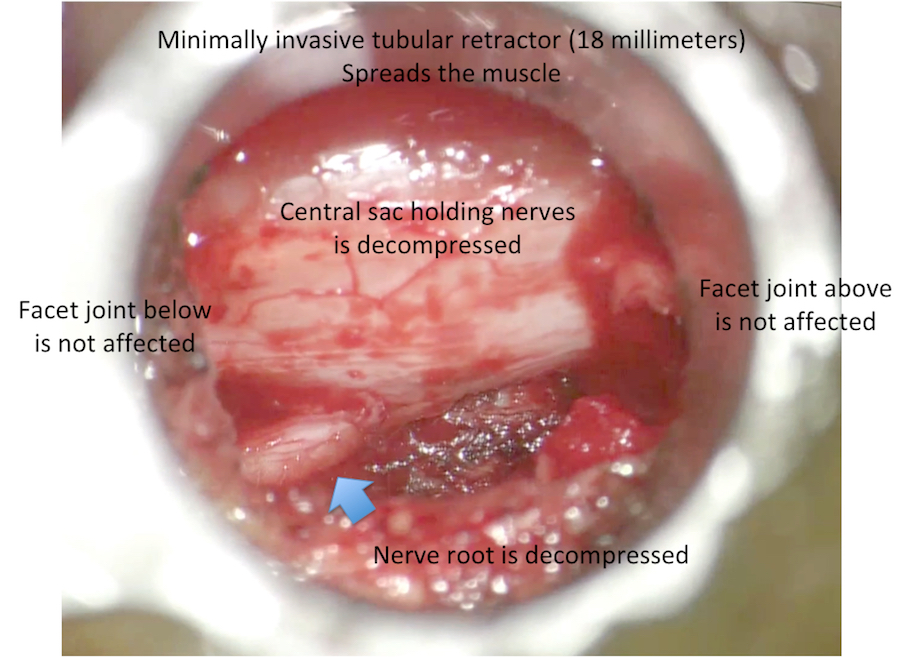
During a minimally invasive tubular lumbar decompression, a tubular retractor dilates the low back muscles, possibly leading to less muscle damage. The joints above and below the decompressed level are not affected.
Spine model showing the minimally invasive tubular dilator spreading the muscle. The muscle is still otherwise attached to the bone, so it’s blood supply is not disrupted and the muscles stay healthy after the procedure. When the tubular dilator is removed after the procedure, the muscle returns to its normal configuration.


Through the tubular retractor, some bone is removed (laminotomy or laminectomy). If a disc herniation, bone spur (osteophyte), synovial cyst, or joint enlargement (facet hypertrophy) is present, the offending cause is removed. The nerves are decompressed. The same procedure, as in the “open” surgery, may be accomplished through a small tube (~18 millimeters).
A minimally invasive tubular lumbar decompression can be performed through a small incision (s) at a single or multiple levels. In certain patients, up to 3 or 4 spinal levels can be decompressed through a single incision that is about 2 centimeters in length.