 Those MIT guys are at it again… Now that they’re banned from blackjack and casinos, they’ve redirected their time to research brain vascular problems… in more minimally invasive ways than ever before.
Those MIT guys are at it again… Now that they’re banned from blackjack and casinos, they’ve redirected their time to research brain vascular problems… in more minimally invasive ways than ever before.
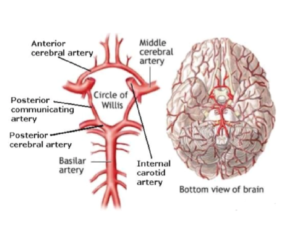
Aneurysms and stroke have long been challenging conditions for neurologists and neurosurgeons to treat. Both arise from blood vessel problems in the brain. The hexagonal network of arteries at the base of the brain, the circle of Willis, has been studied since the mid-1600’s. The word “carotid”, in reference to the carotid artery, is derived from the Greek term- karotide or karos, meaning “to stupefy” or “”plunge into a deep sleep”. For a long time, we’ve known that problems with cerebral arteries cause strokes and neurologic problems.
Surgical treatment for a blocked artery, causing ischemic stroke, originally consisted of “unblocking” the artery through a procedure called a carotid endarterectomy (CEA). CEA is still done today, however it cannot fix smaller arteries in the brain. Thanks to Egas Moniz in the 1970s, cerebral angiography was developed in which small, but somewhat rigid, catheters were advanced from an artery in the groin, up and through the brain vessels. Originally endovascular angiograms were just used to take pictures of the blood vessels. However in 1983, the first endovascular removal of a basilar artery occlusion, causing a stroke, was published. The technique is called thrombectomy. Since, advances in thrombectomy devices make it easier to accomplish. Additionally, medications can now also be administered into a patient’s arm vein, or endovascularly into cerebral arteries, to lyse the blood vessel obstruction. The options we have now seem to work pretty well, but the greatest challenge may be getting the procedure done within about a 3-hour window before the brain cells start to die.
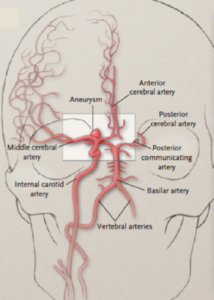 Aneurysms were originally described as, “a lesion having such remote surgical bearings… whether there are surgical indications… further experience alone can tell” (Harvey Cushing). In 1937, the first malleable silver clip was placed over an aneurysm. The clip blocks blood flow to the aneurysm so that it cannot rupture. If the aneurysm has already ruptured, quick treatment is more critical to avoid re-rupture. Great modifications have since occurred to surgical aneurysm clips, and this procedure is also still used today in certain scenarios. The criticism is that who wants their head cut open if there is a less invasive option? Guglielmi started endovascularly detaching platinum coils in aneurysms in 1990. This technique was clearly less invasive than surgically opening a patient’s skull, however the coils only completely blocked off the aneurysms about 38% of the time. Technological advancement ensued, however incomplete blockage of an aneurysm is still the greatest limitation and criticism of endovascular coiling. Not all aneurysms are accessible, using endovascular techniques, either. There has been great debate over the years about whether the surgical risks of clipping an aneurysm or the incomplete treatment risks of coiling an aneurysm, favor one option over the other.
Aneurysms were originally described as, “a lesion having such remote surgical bearings… whether there are surgical indications… further experience alone can tell” (Harvey Cushing). In 1937, the first malleable silver clip was placed over an aneurysm. The clip blocks blood flow to the aneurysm so that it cannot rupture. If the aneurysm has already ruptured, quick treatment is more critical to avoid re-rupture. Great modifications have since occurred to surgical aneurysm clips, and this procedure is also still used today in certain scenarios. The criticism is that who wants their head cut open if there is a less invasive option? Guglielmi started endovascularly detaching platinum coils in aneurysms in 1990. This technique was clearly less invasive than surgically opening a patient’s skull, however the coils only completely blocked off the aneurysms about 38% of the time. Technological advancement ensued, however incomplete blockage of an aneurysm is still the greatest limitation and criticism of endovascular coiling. Not all aneurysms are accessible, using endovascular techniques, either. There has been great debate over the years about whether the surgical risks of clipping an aneurysm or the incomplete treatment risks of coiling an aneurysm, favor one option over the other.
In 2002, the ISAT study convinced many surgeons to favor endovascular treatment. Additionally new devices used to assist coiling were developed, which made some aneurysms that previously were more amenable to clipping, possibly treatable with coiling. This leads to present day, where most aneurysms are endovascularly treated, despite the added complication risk not described in ISAT. Last year, a new study assessed thousands of aneurysms around the world, and found that endovascular coiling was associated with a higher death rate at 2 weeks, compared to surgical clipping. This reminded most of us that aneurysms need to have both endovascular and clipping options considered.
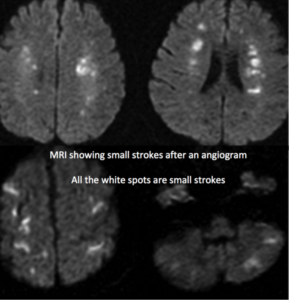
One of the greatest challenges with current cerebral endovascular techniques, for treating stroke or aneurysm, is the catheter’s slight rigidity, and ability to get it to the area needing treatment. The procedure is performed by continuously bumping the catheter into the walls of the blood vessels as the catheter is manipulated to the treatment site. This can dislodge small clots, causing more strokes, or even puncture the artery. There are cases where the cerebral blood vessels are too tortuous that they cannot be navigated to treat a stroke or aneurysm. This is a real problem when “time is brain” for stroke patients. This is a real problem when an aneurysm cannot be accessed for treatment, but could soon re-bleed.
 MIT engineers have recently developed a magnetically steerable catheter that can glide through even the most tortuous labyrinth of blood vessels. The catheter is a nickel- titanium alloy (nitinol), which may be more “bendy” and “springy” than the current option. It is covered in a hydrogel, making it more frictionless and biocompatible. The fact that a magnetic may direct that catheter, as opposed to a surgeon’s hands which uses haptic feedback, smaller corridors may now be accessible. Furthermore the surgeon eventually may not even be present in the room, or the hospital, or the state… In fact, it’s possible this could autonomously driven, negating the need for a human surgeon. Lastly, the catheter is controlled magnetically, which avoids the large doses of radiation currently exposed to the patient and treatment team. Of course, the catheter’s novelty purely resides in getting to the treatment area… this catheter will not affect the challenges in completely coiling an aneurysm.
MIT engineers have recently developed a magnetically steerable catheter that can glide through even the most tortuous labyrinth of blood vessels. The catheter is a nickel- titanium alloy (nitinol), which may be more “bendy” and “springy” than the current option. It is covered in a hydrogel, making it more frictionless and biocompatible. The fact that a magnetic may direct that catheter, as opposed to a surgeon’s hands which uses haptic feedback, smaller corridors may now be accessible. Furthermore the surgeon eventually may not even be present in the room, or the hospital, or the state… In fact, it’s possible this could autonomously driven, negating the need for a human surgeon. Lastly, the catheter is controlled magnetically, which avoids the large doses of radiation currently exposed to the patient and treatment team. Of course, the catheter’s novelty purely resides in getting to the treatment area… this catheter will not affect the challenges in completely coiling an aneurysm.
At least this MIT invention may only infringe on profits of some neuroendovascular surgeons, and not any casino owners.





