 Over 15,000 new spinal cord injuries (SCI) occur each year in the United States. The outcome depends on the severity and location of the injury, resulting in either partial of complete loss of sensory and/or motor function. Partial paralysis occurs about 40% of the time, and complete paralysis about 60% of the time. If a SCI patient survives the first 24 hours, about 80% are still alive at 10 years. First year expenses for patients ranges from $500k to about $1 million. Lifetime costs are multiple millions of dollars.
Over 15,000 new spinal cord injuries (SCI) occur each year in the United States. The outcome depends on the severity and location of the injury, resulting in either partial of complete loss of sensory and/or motor function. Partial paralysis occurs about 40% of the time, and complete paralysis about 60% of the time. If a SCI patient survives the first 24 hours, about 80% are still alive at 10 years. First year expenses for patients ranges from $500k to about $1 million. Lifetime costs are multiple millions of dollars.
Traumatic SCI usually occurs with a sudden blow to or stretching of the spinal cord from either a dislocation, traumatic disc herniation or fractured bone fragments. The spinal cord nerves may be cut or damaged beyond repair, and blood vessels may rupture causing bleeding. Within minutes, the site of injury swells and causes even more
damage. Unfortunately it is this “secondary injury” where a series of cellular, molecular and biochemical phenomena continue to self-destruct the spinal cord tissue, and impede eventual neurologic recovery.
Various treatments have been attempted to limit the long-lasting secondary effects of SCI. After all, the nerves in the spinal cord cannot repair themselves or regenerate.
When indicated, surgical decompression can take the pressure off the spinal cord, but this cannot be achieved quickly enough within the critical minutes following the injury. Furthermore, surgical decompression may not allow enough room for the cord to expand and still avoid injury. Steroids are known to decrease inflammation and swelling, and we have previously tried high dose methylprednisolone in SCI. However this has not shown to provide significant benefit but seems to risk significant side effects. Newer research uses stem cells to regenerate the damaged nerves of the spinal cord. Traditionally, experimental models injected stem cells into the spinal cord at the site of injury, but the needle injection itself may cause more injury. A newer modified delivery method injects in the superficial layers of the spinal cord, or even fluid surrounding the spinal cord, allowing the stem cells to migrate on their own deeper into the cord. Nerve growth factors, like Lin28, are also being shown to help regrow nerve cells in rodent models. Unfortunately, none of this has been very successful in humans.
Recently, some data has indicated other ways to reduce the “secondary injury” following spinal cord trauma. If the swelling of the spinal cord can be diminished, maybe the surrounding blood vessels could continue to supply nutrients and avoid secondary damage. An osmotic transport device (OTD) could create an external osmotic gradient so water could be removed from the spinal cord in a controlled manner.
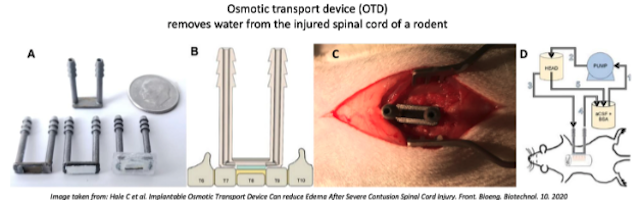 In rodent models, the spinal cord water content significantly elevates as soon as 1 hour after injury and peaks at 72 hours. It remains elevated for about 28 days. Using the OTD surgically implanted on the spinal cord, water content could be reduced by about 1%. While this seems small, significant therapeutic benefits could occur from reducing water content by this small percent. It is difficult to predict the success of this in humans, but is a worthwhile consideration in this otherwise morbid condition.
In rodent models, the spinal cord water content significantly elevates as soon as 1 hour after injury and peaks at 72 hours. It remains elevated for about 28 days. Using the OTD surgically implanted on the spinal cord, water content could be reduced by about 1%. While this seems small, significant therapeutic benefits could occur from reducing water content by this small percent. It is difficult to predict the success of this in humans, but is a worthwhile consideration in this otherwise morbid condition.





