Foot drop is a condition in which the foot cannot elevate (dorsiflex) toward the sky. It can be on one side (unilateral) or both feet (bilateral)
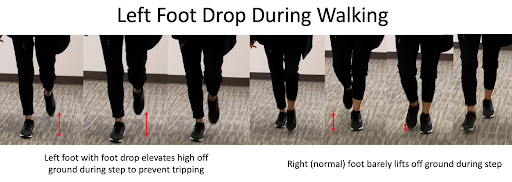 When muscle strength becomes less than a 3 out of 5, an abnormal gait pattern arises, due to the foot tripping on the ground. This is usually called a “steppage gait”. A compensatory hyperflexion in the hip and knee joints, with internal rotation of the foot, prevents the toes from catching on the ground.
When muscle strength becomes less than a 3 out of 5, an abnormal gait pattern arises, due to the foot tripping on the ground. This is usually called a “steppage gait”. A compensatory hyperflexion in the hip and knee joints, with internal rotation of the foot, prevents the toes from catching on the ground.
Injury to the motor pathways of the muscles involved in foot dorsiflexion can occur at any level, from the brain, to the spinal cord, to the peripheral nerves.
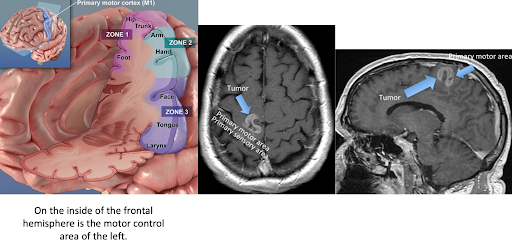 A brain tumor pressing on the leg motor pathways can cause a foot drop, although typically the entire leg may be weak. A right brain lesion could cause a left foot drop.
A brain tumor pressing on the leg motor pathways can cause a foot drop, although typically the entire leg may be weak. A right brain lesion could cause a left foot drop.
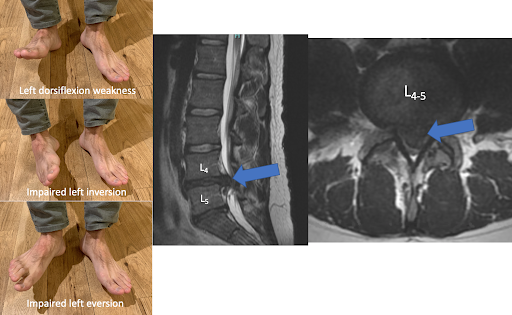
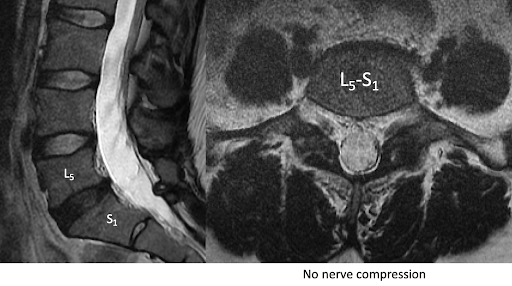
In the lumbar spine, typically the L4 and L5 nerve roots supply the muscles to dorsiflexing the foot. Large disc herniations could cause a left foot drop. From a L4 or L5 radiculopathy, dorsiflexion, foot inversion and foot eversion are all impaired.
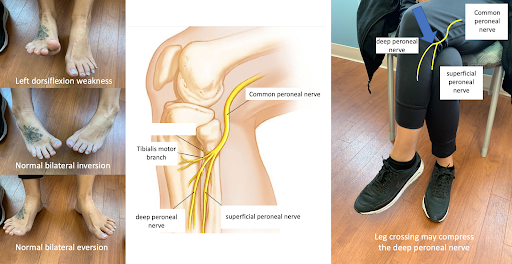
 The peripheral nerves could malfunction, after leaving the spine. The common peroneal nerve supplies the muscles dorsiflexing the foot (anterior tibialis muscle) and everting the foot (peroneus muscles). The superficial peroneal nerve supplies just the muscles everting the foot. The deep peroneal nerve supplies the muscles dorsiflexing. In this particular case, the patient cannot dorsiflex, but can invert and evert the foot, suggesting a deep peroneal nerve problem from crossing the legs and compression of the nerve at the fibular bone head.
The peripheral nerves could malfunction, after leaving the spine. The common peroneal nerve supplies the muscles dorsiflexing the foot (anterior tibialis muscle) and everting the foot (peroneus muscles). The superficial peroneal nerve supplies just the muscles everting the foot. The deep peroneal nerve supplies the muscles dorsiflexing. In this particular case, the patient cannot dorsiflex, but can invert and evert the foot, suggesting a deep peroneal nerve problem from crossing the legs and compression of the nerve at the fibular bone head.
Most commonly in the neurosurgical practice, we see nerve compression in the spine. Spontaneous resolution of foot drop can occur with just observation of a disc herniation. In other cases, therapy, injections or even surgery are used. Brain tumors pressing directly on the leg motor area is probably the most rare occurrence. However, neurosurgeons must use a detailed neurologic exam to identify peripheral nerve compression. This is not the most typical patient we see, but not uncommon either. In identifying which muscle groups are impaired, diagnosing a peripheral compressive neuropathy can be predicted even without a MRI. However, MRI will usually show no nerve compression if ordered.
Foot drop is a condition in which the foot cannot elevate (dorsiflex) toward the sky. It can be on one side (unilateral) or both feet (bilateral).
When muscle strength becomes less than a 3 out of 5, an abnormal gait pattern arises, due to the foot tripping on the ground. This is usually called a “steppage gait”. A compensatory hyperflexion in the hip and knee joints, with internal rotation of the foot, prevents the toes from catching on the ground.
 Injury to the motor pathways of the muscles involved in foot dorsiflexion can occur at any level, from the brain, to the spinal cord, to the peripheral nerves.
Injury to the motor pathways of the muscles involved in foot dorsiflexion can occur at any level, from the brain, to the spinal cord, to the peripheral nerves.
A brain tumor pressing on the leg motor pathways can cause a foot drop, although typically the entire leg may be weak. A right brain lesion could cause a left foot drop.
In the lumbar spine, typically the L4 and L5 nerve roots supply the muscles to dorsiflexing the foot. Large disc herniations could cause a left foot drop. From a L4 or L5 radiculopathy, dorsiflexion, foot inversion and foot eversion are all impaired.
The peripheral nerves could malfunction, after leaving the spine. The common peroneal nerve supplies the muscles dorsiflexing the foot (anterior tibialis muscle) and everting the foot (peroneus muscles). The superficial peroneal nerve supplies just the muscles everting the foot. The deep peroneal nerve supplies the muscles dorsiflexing. In this particular case, the patient cannot dorsiflex, but can invert and evert the foot, suggesting a deep peroneal nerve problem from crossing the legs and compression of the nerve at the fibular bone head.
 Most commonly in the neurosurgical practice, we see nerve compression in the spine. Spontaneous resolution of foot drop can occur with just observation of a disc herniation. In other cases, therapy, injections or even surgery are used. Brain tumors pressing directly on the leg motor area is probably the most rare occurrence. However, neurosurgeons must use a detailed neurologic exam to identify peripheral nerve compression. This is not the most typical patient we see, but not uncommon either. In identifying which muscle groups are impaired, diagnosing a peripheral compressive neuropathy can be predicted even without a MRI. However, MRI will usually show no nerve compression if ordered.
Most commonly in the neurosurgical practice, we see nerve compression in the spine. Spontaneous resolution of foot drop can occur with just observation of a disc herniation. In other cases, therapy, injections or even surgery are used. Brain tumors pressing directly on the leg motor area is probably the most rare occurrence. However, neurosurgeons must use a detailed neurologic exam to identify peripheral nerve compression. This is not the most typical patient we see, but not uncommon either. In identifying which muscle groups are impaired, diagnosing a peripheral compressive neuropathy can be predicted even without a MRI. However, MRI will usually show no nerve compression if ordered.





