Newer studies may show more seizure improvement over time.
A VNS device is unlikely to completely stop seizures. The main goal is to diminish seizures and medication use. Historically, patients could expect about 20-30% improvement in seizures in the first 3-6 months, which could increase up to 40-50% improvement after a few years. Newer studies may show more seizure improvement over time. There may be up to 75% reduction is seizure frequency at 10 years. Unfortunately, there is no way to predict a success rate prior to surgery.
It should also be noted what we mean by seizure improvement. Epilepsy outcome is often classified on a scale. Engel class I outcome is often thought to be complete seizure freedom or rare non-disabling seizures. Engel class II outcome is often thought to be >90% seizure frequency reduction. Engel class III outcome is ~50-90% reduction. Engel class IV is less than 50% reduction. Engel class V is no reduction. Engel class I is rarely achieved.
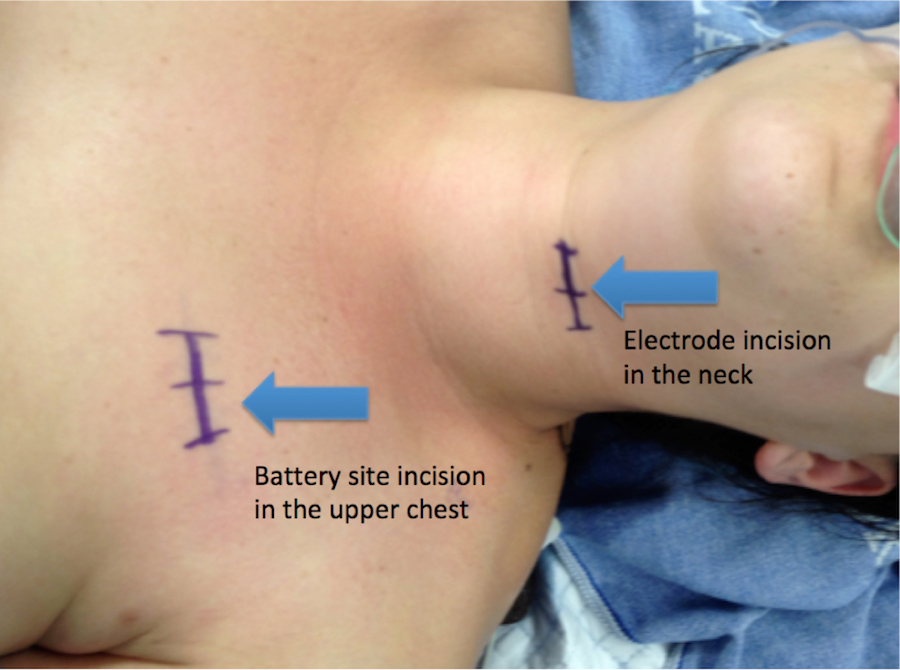
A VNS device is compatible with brain MRIs, however recipients cannot undergo body MRIs following the procedure.
If you have questions about epilepsy surgery, contact our BOARD CERTIFIED surgeon at Rocky Mountain Brain & Spine Institute.